


 Sign Out
Sign Out

Pharmacology: Pharmacodynamics: Mechanism of action: Pathological changes in dementia such as Alzheimer's Disease involve cholinergic neuronal pathways that project from the basal forebrain to the cerebral cortex and hippocampus. These pathways are known to be involved in attention, learning and memory and other cognitive processes. Rivastigmine, a brain-selective acetyl- and butyryl-cholinesterase inhibitor of the carbamate type, is thought to facilitate cholinergic neurotransmission by slowing the degradation of acetylcholine released by functionally intact cholinergic neurons. Data from animal studies indicate that rivastigmine selectively increases the availability of acetylcholine in the cortex and hippocampus. Thus, Exelon may have an ameliorative effect on cholinergic-mediated cognitive deficits associated with Alzheimer's Disease and with Parkinson's disease. In addition, there is some evidence that cholinesterase inhibition could slow the formation of amyloidogenic beta-amyloid-precursor protein (APP) fragments, and thus of amyloid plaques, which are one of the main pathological features of Alzheimer's Disease.
Rivastigmine interacts with its target enzymes by forming a covalently bound complex that temporarily inactivates the enzymes. In healthy young men, an oral 3.0 mg dose decreases acetylcholinesterase (AChE) activity in cerebro spinal fluid (CSF) by approximately 40% within the first 1.5 hours after administration. Activity of the enzyme returns to baseline levels about 9 hours after the maximum inhibitory effect has been achieved. Butyrylcholinesterase (BuChE) activity in CSF was transiently inhibited and was no longer different from baseline after 3.6 hours in healthy young volunteers. In patients with Alzheimer's Disease (AD), inhibition of acetylcholinesterase in CSF by rivastigmine was dose-dependent up to 6 mg given twice daily, the highest dose tested. Inhibition of BuChE activity in CSF of AD patients by rivastigmine was similar to that of AchE, with a change from baseline of more than 60% after 6 mg given twice daily. The effect of rivastigmine on AChE and BuChE activity in CSF was sustained after 12 months administration, the longest time studied. Statistically significant correlations were found between the degree of inhibition by rivastigmine of AChE and BuChE in the CSF and changes on a compound measure of cognitive performance in AD patients; however, only BuChE inhibition in CSF was significantly and consistently correlated with improvements in speed-, attention- and memory-related subtests.
Clinical Studies: Clinical studies in Alzheimer's Dementia: The efficacy of Exelon patches (10, 15 and 20) in patients with mild to moderately severe dementia of the Alzheimer's type has been demonstrated in a 24-week double-blind, placebo-controlled core study and its open-label extension phase and in a 48-week double blind active comparator study.
The efficacy of Exelon patch 15 in patients with severe dementia of the Alzheimer's type has been demonstrated in a 24-week double-blind study.
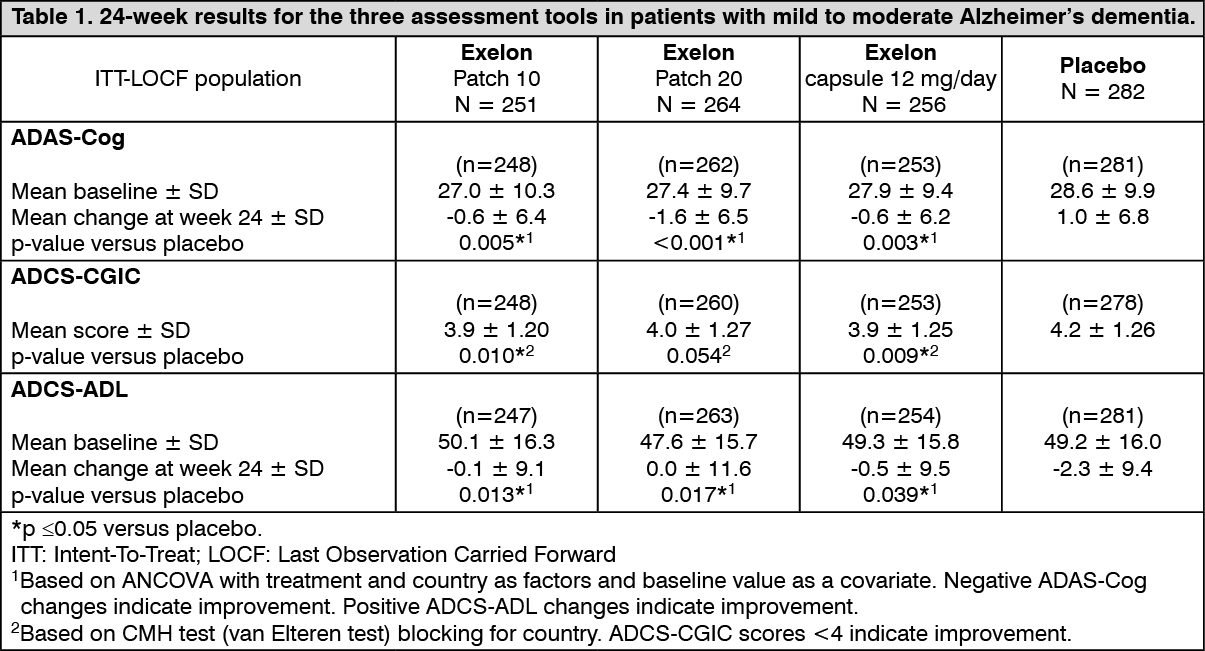
Mild to moderate Alzheimer's dementia: 24-week controlled studies: Patients involved in a placebo-controlled study had an MMSE (Mini-Mental State Examination) score of 10 to 20. Efficacy was established by the use of independent, domain-specific assessment tools which were applied at regular intervals during the 24-week treatment period. These include the ADAS-Cog (a performance-based measure of cognition), the ADCS-CGIC (Alzheimer's Disease Cooperative Study-Clinician's Global Impression of Change: a comprehensive global assessment of the patient by the physician incorporating caregiver input), and the ADCS-ADL (a caregiver-rated assessment of the activities of daily living including personal hygiene, feeding, dressing, household chores such as shopping, retention of ability to orient oneself to surroundings as well as involvement in activities related to finances). The 24-week results for the three assessment tools are summarized in Table 1. (See Table 1.)
 Click on icon to see table/diagram/image
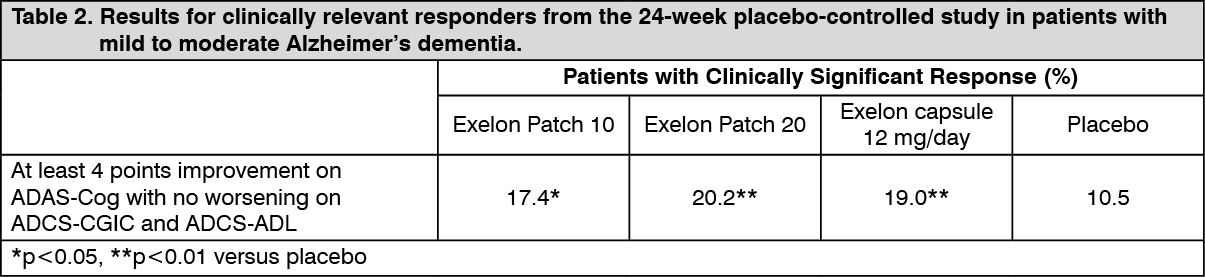
Click on icon to see table/diagram/imageThe results for clinically relevant responders from the 24-week study are provided in Table 2. Clinically relevant improvement was defined a priori as at least 4-point improvement on the ADAS-cog, no worsening on the ADCS-CGIC, and no worsening on the ADCS-ADL. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageSimilar results were observed with Exelon Patch 10 in separately conducted controlled studies in Chinese and Japanese patients with mild to moderately severe Alzheimer's dementia.
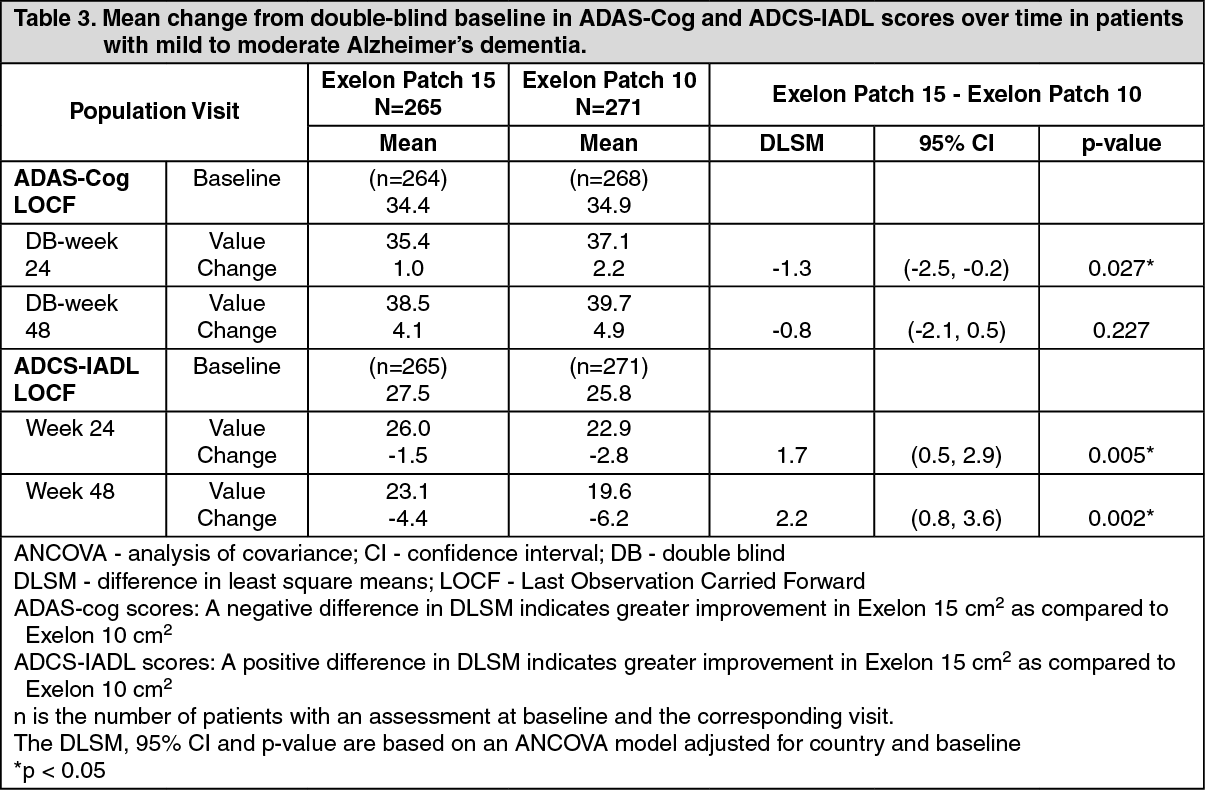
48-week active comparator-controlled study: Patients involved in the active comparator-controlled study had an initial baseline MMSE (Mini-Mental State Examination) score of 10 to 24. The study was designed to compare the efficacy of the Exelon Patch 15 versus the Exelon Patch 10 during a 48-week double blind treatment phase in Alzheimer's disease patients who demonstrated functional and cognitive decline after an initial 24 to 48-week open-label treatment phase while on a maintenance dose of Exelon Patch 10. Functional decline was assessed by the investigator and cognitive decline was defined as a decrease in the MMSE score of ≥2 points from the previous visit or a decrease of ≥3 points from baseline. Efficacy was established by the use of independent, domain-specific assessment tools which were applied at regular intervals during the 48-week treatment period. These include the ADAS-Cog (a performance-based measure of cognition) and the ADCS-instrumental ADL (a subscale from the ADCS-ADL activities of daily living scale assessing instrumental activities which are thought to involve more complex cognitive activities and represent clinically meaningful functional activities of daily living, which include maintaining finances, meal preparation, shopping, ability to orient oneself to surroundings, able to be left unattended, etc.). The 48-week results for the two assessment tools are summarized in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
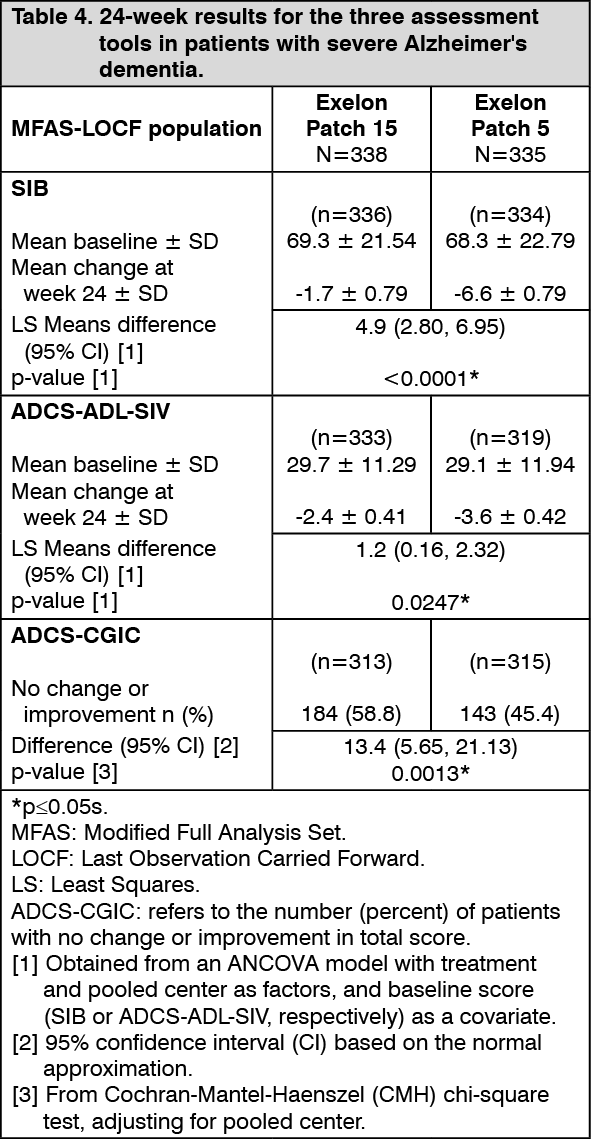
Click on icon to see table/diagram/imageSevere Alzheimer's dementia: 24-week controlled study: Patients involved in the controlled study had at baseline an MMSE (Mini-Mental State Examination) score of ≥3 and ≤12. The study was designed to compare the efficacy of Exelon Patch 15 versus Exelon Patch 5 during a 24-week double blind treatment phase in severe Alzheimer's disease. Efficacy was established by the use of independent, domain-specific assessment tools. These include the SIB, the ADCS-ADL-SIV and the ADCS-CGIC.
The SIB: the Severe Impairment Battery is a 40-item scale with a range of possible scores from 0 to 100, with higher scores reflecting higher levels of cognitive function.
The ADCS-ADL-SIV: the Alzheimer's Disease Cooperative Study Activity of Daily Living-Severe Impairment Version is a caregiver-based scale consisting of 19 items designed to assess the patient's performance of both basic and instrumental activities of daily living, which had been used in several studies in moderate to severe Alzheimer's dementia. The total score ranges from 0 - 54, with higher scores indicating better function.
The ADCS-CGIC: the Alzheimer's Disease Cooperative Study-Clinical Global Impression of Change is a comprehensive global assessment of the patient by the physician incorporating caregiver input.
The 24-week results for the three assessment tools are summarized in Table 4. (See Table 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageClinical studies in dementia associated with Parkinson's disease: The efficacy of Exelon capsules in dementia associated with Parkinson's disease was demonstrated in a 24-week multicenter, double-bind, placebo-controlled core study and its 24-week open-label extension phase. Patients involved in this study were to have an MMSE (Mini-Mental State Examination) score at screening of 10 to 26. Efficacy has been established by the use of two independent scales which were assessed at regular intervals during a 6-month treatment period: the ADAS-Cog, a measure of cognition, and the global measure ADCS-CGIC.
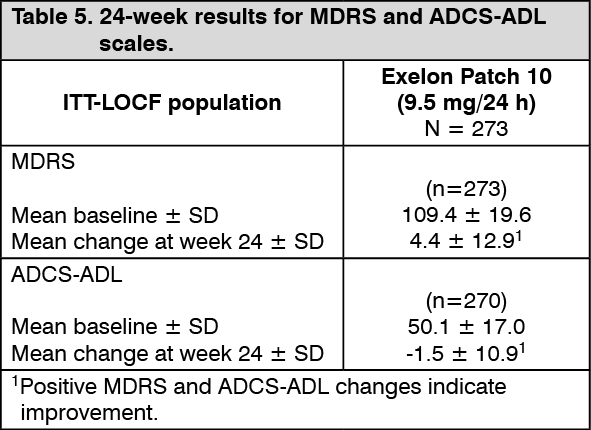
The efficacy of Exelon transdermal patch in dementia associated with Parkinson's disease was investigated in an open-label safety study. Patients involved in this study were to have an MMSE score at screening of 10 to 26. Efficacy was evaluated by the use of two independent scales which were assessed at regular intervals. These include the MDRS (Mattis Dementia Rating Scale, a performance-based measure of cognition) and the ADCS-ADL.
The 24-week results for the two scales are summarized in Table 5. (See Table 5.)
 Click on icon to see table/diagram/image
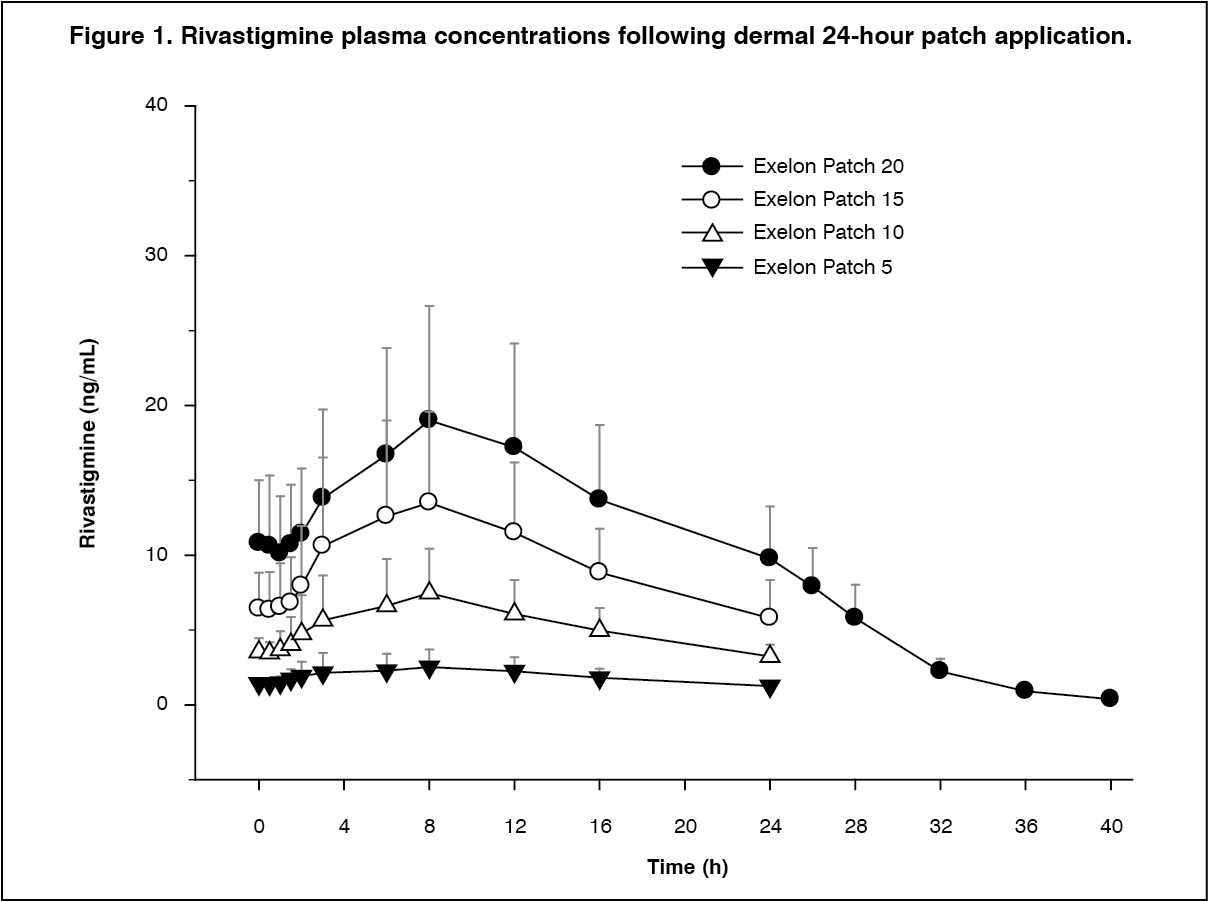
Click on icon to see table/diagram/imagePharmacokinetics: Absorption: Absorption of rivastigmine from Exelon patches is slow. After the first dose, detectable plasma concentrations are observed after a lag time of 0.5 to 1 hour. Concentrations then rise slowly and typically after 8 hours reach levels close to maximum, although maximum values (Cmax) are often reached at later times (10 to 16 hours). After the peak, plasma concentrations slowly decrease over the remainder of the 24-hour period of application. With multiple dosing (such as at steady state), after the previous patch is replaced with a new one, plasma concentrations initially decrease slowly for about 40 min on average, until absorption from the newly applied patch becomes faster than the elimination, and plasma levels begin to rise again to reach a new peak at approximately 8 hours. At steady state, trough levels are approximately 50% of peak levels, in contrast to oral dosing, with which concentrations fall off to virtually zero between doses (see Figures 1 and 2). This time course of plasma concentrations is observed with all patch strengths (sizes) in the investigated range of Exelon Patch 5 to Exelon Patch 20. Although less pronounced than with the oral formulation, exposure to rivastigmine (Cmax and AUC) increased over-proportionally with rising patch doses. Escalating from Exelon Patch 5 to Exelon Patch 20, the increase in rivastigmine AUC relative to the lowest dose of Exelon Patch 5 was 2.6, 4.9 and 7.8-fold for Exelon Patch 10, Exelon Patch 15 and Exelon Patch 20, respectively. The fluctuation index (FI), i.e., a measure of the relative difference between peak and trough concentrations ((Cmax to Cmin)/Cavg), was in the range 0.57 to 0.77 for the patch, thus demonstrating a much smaller fluctuation between trough and peak concentrations than for the oral formulation (FI = 3.96 to 6.24). As determined by compartmental modeling the Exelon Patch 20 exhibited exposure (AUC24h) in a typical patient equivalent to that which would be provided by an oral dose of about 9 to 10 mg twice daily (i.e., 18 to 20 mg/day), while Exelon Patch 10 exhibited exposure equivalent to that provided by an oral dose of about 6 mg twice daily (i.e., 12 mg/day). (See Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image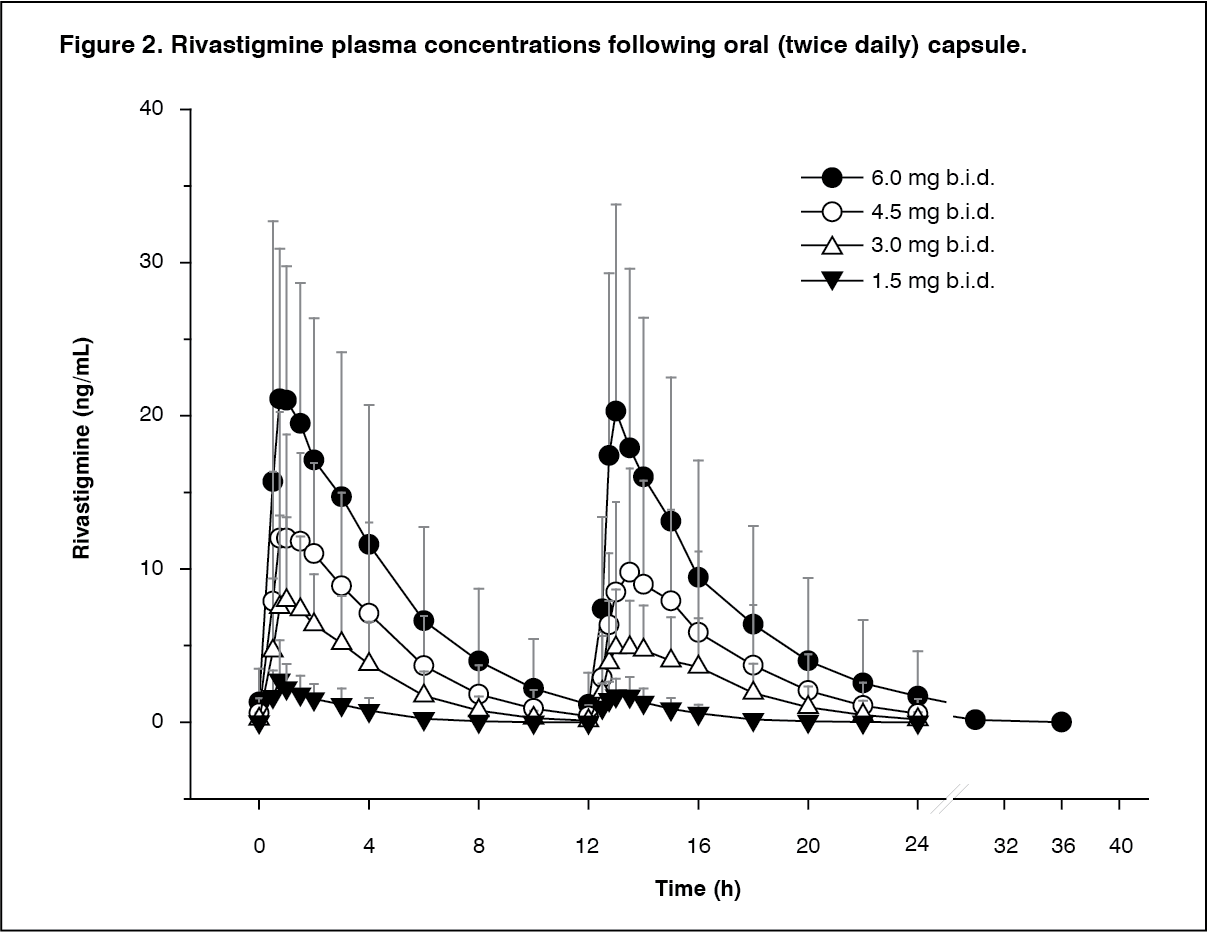 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageIn a single dose study directly comparing the patch versus oral administration, the inter-subject variability in rivastigmine pharmacokinetic parameters (normalized to dose/kg bodyweight) was 43% (Cmax) and 49% (AUC0-24h) after the patch versus 74% and 103%, respectively, after the oral capsule. Similarly, inter-subject variability in rivastigmine pharmacokinetic parameters was lower after the patch than after the oral capsule in a steady-state study in Alzheimer's dementia patients given repeated doses. The inter-patient variability was at most 45% (Cmax) and 43% (AUC0-24h) after the patch, while 71% and 73%, respectively, after the oral form.
A relationship between drug exposure at steady state (rivastigmine and metabolite NAP226-90) and bodyweight was observed in Alzheimer's dementia patients. Compared to a patient with a body weight of 65 kg, the rivastigmine steady-state concentrations in a patient with a body weight of 35 kg would be approximately doubled, while for a patient with a body weight of 100 kg the concentrations would be approximately halved. The effect of bodyweight on drug exposure suggests special attention to patients with very low body weight during up-titration (see DOSAGE & ADMINISTRATION).
Rivastigmine was well released from the transdermal system over a 24-hour dermal application with approximately 50% of the drug load released from the system.
Exposure (AUC∞) to rivastigmine (and metabolite NAP266-90) was highest when the patch was applied to the upper back, chest, or upper arm. Two other sites (abdomen and thigh) could be used if none of the three other sites is available, but the practitioner should keep in mind that the rivastigmine plasma exposure associated with these sites was approximately 20-30% lower.
There was no relevant accumulation of rivastigmine or the metabolite NAP226-90 in plasma in patients with Alzheimer's disease, except that with patch treatment plasma levels on the second day were higher than on the first.
The pharmacokinetic profile of rivastigmine transdermal patches was comparable in patients with Alzheimer's disease and in patients with dementia associated with Parkinson's disease.
Distribution: Rivastigmine is weakly bound to plasma proteins (approximately 40%). It readily crosses the blood-brain barrier and has an apparent volume of distribution in the range of 1.8 to 2.7 l/kg.
Metabolism: Rivastigmine is rapidly and extensively metabolized with an apparent elimination half-life in plasma of approximately 3.4 hours after patch removal. Elimination was absorption rate limited (flip-flop kinetics), which explains the longer t½ after patch (3.4 h) versus oral or i.v. administrations (1.4 to 1.7 h). Metabolism is primarily via cholinesterase-mediated hydrolysis to the decarbamylated metabolite. In vitro, this metabolite shows minimal inhibition of acetylcholinesterase (<10%). Based on in vitro studies, no pharmacokinetic drug interactions are expected with drugs metabolized by the following cytochrome isoenzymes: CYP1A2, CYP2D6, CYP3A4/5, CYP2E1, CYP2C9, CYP2C8, CYP2C19, or CYP2B6. Based on evidence from animal studies, the major cytochrome P450 isoenzymes are minimally involved in rivastigmine metabolism. Total plasma clearance of rivastigmine was approximately 130 liters/h after a 0.2 mg intravenous dose and decreased to 70 liters/h after a 2.7 mg intravenous dose, which is consistent with the non-linear, over proportional pharmacokinetics of rivastigmine due to saturation of its elimination.
The metabolite-to-parent AUC∞ ratio was around 0.7 after patch versus 3.5 after oral administration, indicating that much less metabolism occurred after dermal treatment. Less NAP226-90 is formed following patch application, presumably because of the lack of pre-systemic (hepatic first pass) metabolism.
Elimination: Unchanged rivastigmine is found in trace amounts in the urine; renal excretion of the metabolites is the major route of elimination. Following administration of 14C-rivastigmine, renal elimination was rapid and essentially complete (>90%) within 24 hours. Less than 1% of the administered dose is excreted in the faeces.
Elderly subjects: Age had no impact on the exposure to rivastigmine in Alzheimer's disease patients treated with Exelon patches.
Subjects with hepatic impairment: No study was conducted with the Exelon patches in subjects with hepatic impairment. After oral administration, the Cmax of rivastigmine was approximately 60% higher and the AUC of rivastigmine was more than twice as high in subjects with mild to moderate hepatic impairment than in healthy subjects. Following a single 3-mg oral dose or multiple 6-mg twice a day oral doses, the mean oral clearance of rivastigmine was approximately 60 to 65% lower in mild (n=7, Child-Pugh score 5 to 6) and moderate (n=3, Child-Pugh score 7 to 9) hepatically impaired patients (n=10, biopsy proven) than in healthy subjects (n=10). These pharmacokinetic changes had no effect on either the incidence or severity of adverse effects (see DOSAGE & ADMINISTRATION and PRECAUTIONS).
Subjects with renal impairment: No study was conducted with the Exelon patches in subjects with renal impairment. Based on population analysis creatinine clearance did not show any clear effect on steady state concentrations of rivastigmine or its metabolite. No dosage adjustment is necessary in patients with renal impairment (see DOSAGE & ADMINISTRATION).
Toxicology: Non-Clinical Safety Data: Acute toxicity: The estimated oral LD50 values in mice were 5.6 mg base/kg (males) and 13.8 mg base/kg (females). The estimated oral LD50 values in rats were 8.1 mg base/kg (males) and 13.8 mg base/kg (females).
Repeated dose toxicity: Oral and topical repeated-dose toxicity studies in mice, rats, rabbits, dogs and minipigs revealed only effects associated with an exaggerated pharmacological action. No target organ toxicity was observed. Oral and topical dosing in animal studies was limited due to the sensitivity of the animal models used.
Mutagenicity: Rivastigmine was not mutagenic in in vitro tests for gene mutations and primary DNA damage. In tests for chromosomal damage in vitro, a small increase in the number of cells carrying chromosomal aberrations occurred at very high concentrations. However, as there was no evidence of clastogenic activity in the more relevant in vivo micronucleus test assessing chromosomal damage, it is most likely that the in vitro findings were false positive observations. In addition, the major metabolite NAP226-90 did not induce structural chromosome aberrations in an in vitro test indicating that the compound has no genotoxic potential.
Carcinogenicity: No evidence of carcinogenicity was found in oral and topical studies in mice and in an oral study in rats at the maximum tolerated dose. The exposure to rivastigmine and its metabolites was approximately equivalent to human exposure with highest doses of rivastigmine capsules and patches.
Reproductive toxicity: see PREGNANCY, LACTATION, FEMALES AND MALES OF REPRODUCTIVE POTENTIAL under Use in Pregnancy & Lactation).
Local tolerance: Rivastigmine patches were not phototoxic and considered to be a non-sensitizer. In some other dermal toxicity studies, a mild irritant effect on the skin of laboratory animals, including controls, was observed. This may indicate a potential for Exelon patches to induce mild erythema in patients. A mild eye/mucosal irritation potential of rivastigmine was identified in a rabbit study (see Important administration instructions under DOSAGE & ADMINISTRATION).